1. Advocates for clients who have been neglected or underrepresented in the system.
During my outpatient pediatric rotation, it was vital to have the ability to collaborate with clients and caregivers present in the room in order to provide the best plan of care that the client required. There were many times in which the main concern for the caregiver and the client were not directly related to occupational therapy services, but instead they needed a healthcare professional to help guide them through the difficulties that come up in the medical world. This scenario would commonly occur with my Spanish speaking families that were unable to properly communicate their concerns due to lack of a medical translator and not having the time or place to really dive into issues. Due to the language barrier and the scarce amount of medical translators available, these clients are overwhelmingly underrepresented in the system and sometimes are even put on the back burner with their medical concerns based on implicit biases. Even though as an occupational therapist in an outpatient clinic setting I am tasked to base my therapy services on related goals. However, if the client does not have their basic needs met, then I must address those within my session. I had a client on my case at my outpatient pediatric rotation that had a chronic iron deficiency disorder and they currently were unable to get any of this substance from food due to also having sensory processing issues with foods. In order to address everything all within a one hour therapy session, my clinical instructor and I would split up the concerns of the client and caregiver. I would use the skills I had to address the therapy related concerns of oral aversions through leading the feeding session by myself, while my clinical instructor would use her expertise to call doctors and use the bilingual speech language pathologist as a translator in order to provide overall holistic care to the client and caregivers. The caregiver was very appreciative and greatly valued that we took the time to listen to their problems and take the time to actually assist them, rather than passing their issues around until they finally hit a dead end. As a future occupational therapist we must advocate for and be the representation for our clients regardless of their medical situation or educational background. If we do not stop to help then who knows if they will ever receive the care and attention that they deserve.
Below is a discussion board post from my experience:
During my outpatient pediatric rotation, it was vital to have the ability to collaborate with clients and caregivers present in the room in order to provide the best plan of care that the client required. There were many times in which the main concern for the caregiver and the client were not directly related to occupational therapy services, but instead they needed a healthcare professional to help guide them through the difficulties that come up in the medical world. This scenario would commonly occur with my Spanish speaking families that were unable to properly communicate their concerns due to lack of a medical translator and not having the time or place to really dive into issues. Due to the language barrier and the scarce amount of medical translators available, these clients are overwhelmingly underrepresented in the system and sometimes are even put on the back burner with their medical concerns based on implicit biases. Even though as an occupational therapist in an outpatient clinic setting I am tasked to base my therapy services on related goals. However, if the client does not have their basic needs met, then I must address those within my session. I had a client on my case at my outpatient pediatric rotation that had a chronic iron deficiency disorder and they currently were unable to get any of this substance from food due to also having sensory processing issues with foods. In order to address everything all within a one hour therapy session, my clinical instructor and I would split up the concerns of the client and caregiver. I would use the skills I had to address the therapy related concerns of oral aversions through leading the feeding session by myself, while my clinical instructor would use her expertise to call doctors and use the bilingual speech language pathologist as a translator in order to provide overall holistic care to the client and caregivers. The caregiver was very appreciative and greatly valued that we took the time to listen to their problems and take the time to actually assist them, rather than passing their issues around until they finally hit a dead end. As a future occupational therapist we must advocate for and be the representation for our clients regardless of their medical situation or educational background. If we do not stop to help then who knows if they will ever receive the care and attention that they deserve.
Below is a discussion board post from my experience:
2. Fulfills commitments to the professional community.
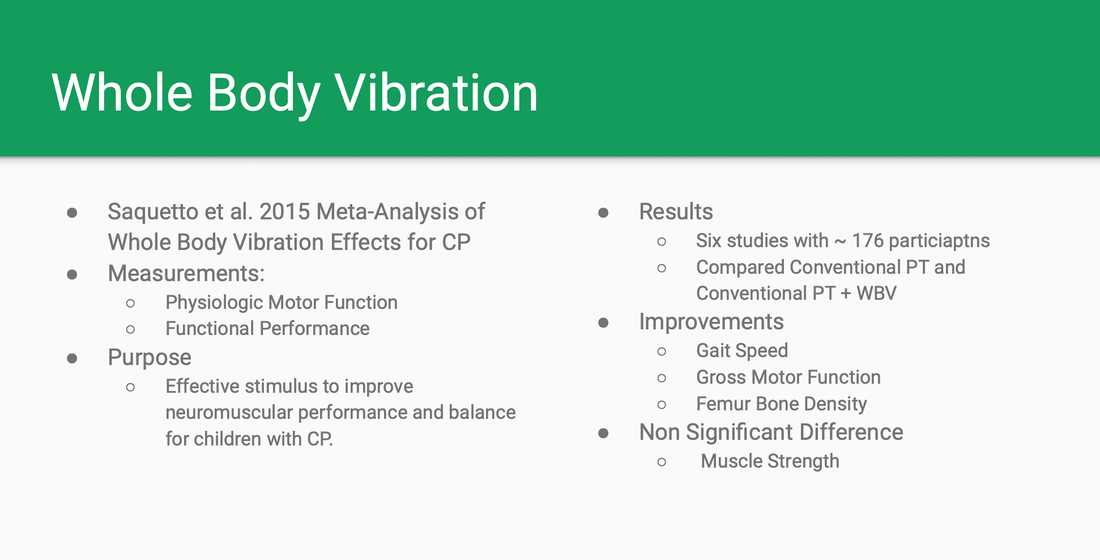
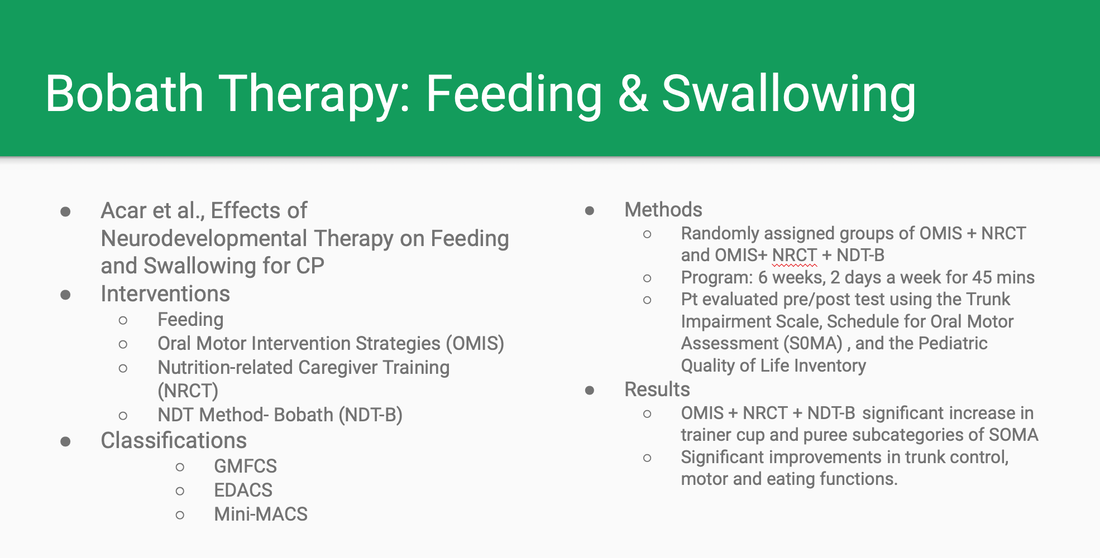
As a future occupational therapist, it is my duty to remain committed to the professional community in order to put forward the best of care to my clients and continue to foster the bonds with other clinicians. At my outpatient pediatric rotation, I had the opportunity to present an in-service topic about resources for therapists in regards to the clients who were diagnosed with Cerebral Palsy. The focus on this in-service was to gather valuable resources through utilizing classification systems, emerging areas of treatment, and adaptive products to aide clients that had Cerebral Palsy due to the varying strengthens and weakness that each child had. In order to incorporate the entire professional community consisting of other disciplines of therapists, I had included resources that addressed the physical, social, and nutritional aspects that influence a client's occupational performance in order to create a more holistic treatment approach. For children with Cerebral Palsy there are a multitude of classification systems that are used across the medical field, and it is important that an occupational therapist considers more than just the systems that relate to use the upper extremities. During my in-service I broke down the classification systems into each related therapy discipline and provided the clinic with examples of when they could utilize a system that is not directly within their scope of practice. For example, one of my clients with Cerebral Palsy was unable to communicate verbally and had to use a communication device in order to inform me which toy they wanted to reach. Even though I am not a Speech Language Pathologist, I know as a future occupational therapist that giving the client a voice in any and all aspects is motivating and allows for them to better participate in their own therapy progress. In the next section of my in-service I went into the evidence based research that I had discovered. I discussed the effects on these new findings, and considered how to incorporate these findings into other professions. Since a majority of the clients that have Cerebral Palsy receive therapy through a co-treatment set-up, I provided new evidence based research that could integrate physical and occupational therapy, as well as occupational and speech therapy. Through my findings I had the ability to share with the professional community new findings on utilizing whole body vibration to increase postural control and implementing the Bobath therapy into feeding sessions for a greater intake of nutrition. Following these emerging treatments, the final resource I provided was adaptive products from the Cerebral Palsy Foundation that promoted out of the box thinking that could increase occupational, physical, and social performance in a child with this diagnosis. This in-service overlapped the gaps that we can face in the professional community. It is important to understand more in-depth about other disciplines for each therapist to provide ethically based resources to treat clients to the full holistic extent.
As a future occupational therapist, it is my duty to remain committed to the professional community in order to put forward the best of care to my clients and continue to foster the bonds with other clinicians. At my outpatient pediatric rotation, I had the opportunity to present an in-service topic about resources for therapists in regards to the clients who were diagnosed with Cerebral Palsy. The focus on this in-service was to gather valuable resources through utilizing classification systems, emerging areas of treatment, and adaptive products to aide clients that had Cerebral Palsy due to the varying strengthens and weakness that each child had. In order to incorporate the entire professional community consisting of other disciplines of therapists, I had included resources that addressed the physical, social, and nutritional aspects that influence a client's occupational performance in order to create a more holistic treatment approach. For children with Cerebral Palsy there are a multitude of classification systems that are used across the medical field, and it is important that an occupational therapist considers more than just the systems that relate to use the upper extremities. During my in-service I broke down the classification systems into each related therapy discipline and provided the clinic with examples of when they could utilize a system that is not directly within their scope of practice. For example, one of my clients with Cerebral Palsy was unable to communicate verbally and had to use a communication device in order to inform me which toy they wanted to reach. Even though I am not a Speech Language Pathologist, I know as a future occupational therapist that giving the client a voice in any and all aspects is motivating and allows for them to better participate in their own therapy progress. In the next section of my in-service I went into the evidence based research that I had discovered. I discussed the effects on these new findings, and considered how to incorporate these findings into other professions. Since a majority of the clients that have Cerebral Palsy receive therapy through a co-treatment set-up, I provided new evidence based research that could integrate physical and occupational therapy, as well as occupational and speech therapy. Through my findings I had the ability to share with the professional community new findings on utilizing whole body vibration to increase postural control and implementing the Bobath therapy into feeding sessions for a greater intake of nutrition. Following these emerging treatments, the final resource I provided was adaptive products from the Cerebral Palsy Foundation that promoted out of the box thinking that could increase occupational, physical, and social performance in a child with this diagnosis. This in-service overlapped the gaps that we can face in the professional community. It is important to understand more in-depth about other disciplines for each therapist to provide ethically based resources to treat clients to the full holistic extent.
|
|
3. Represents the unique perspective of occupational therapy when participating in inter-professional situations.
When working in an inpatient rehabilitation hospital there is always an opportunity to represent the unique perspective of occupational therapy within an inter-professional situation. At my inpatient rotation, each occupational therapist is paired with a physical therapist to share a caseload in order to provide the most consistent plan of care with a minimal amount of transferring between different therapists. I had the ability to work with my clinical instructor's partnered physical therapist throughout my clinical rotation. We would collaborate together on when to work with clients, or share any information we had gathered related to an evaluation or treatment session. There would always be an opportunity with my physical therapy partner to discuss what functional activities that could better our client's skills and alternating between days on more intensive based treatment session for those client working on walking or standing. The physical therapist partner would also assist with transfers that required more than one person and they would provide the biomechanics strategies to improve posture and balance while I could focus on addressing any concerns of the patients regarding toileting, dressing, or bathing. Having a partner in another discipline is also beneficial when addressing clients that may not be compliant or appreciative of occupational therapy services, as my partner would always stand up for our profession and would never let a client speak poorly about occupational therapy. I improved my communication as well as advocation skills through working with my clinical instructor and physical therapy partner. As a future occupational therapist at an inpatient rotation, I gained the ability to communicate and advocate for the profession through an inter-professional situation. I am now more prepared to enter the workforce after completing this rotation. These are vital skills that I will carry into my career when I become a practicing occupational therapist in the medical field while working with other healthcare professionals.
Below is a comment on my Final Fieldwork Evaluation from my clinical instructor:
When working in an inpatient rehabilitation hospital there is always an opportunity to represent the unique perspective of occupational therapy within an inter-professional situation. At my inpatient rotation, each occupational therapist is paired with a physical therapist to share a caseload in order to provide the most consistent plan of care with a minimal amount of transferring between different therapists. I had the ability to work with my clinical instructor's partnered physical therapist throughout my clinical rotation. We would collaborate together on when to work with clients, or share any information we had gathered related to an evaluation or treatment session. There would always be an opportunity with my physical therapy partner to discuss what functional activities that could better our client's skills and alternating between days on more intensive based treatment session for those client working on walking or standing. The physical therapist partner would also assist with transfers that required more than one person and they would provide the biomechanics strategies to improve posture and balance while I could focus on addressing any concerns of the patients regarding toileting, dressing, or bathing. Having a partner in another discipline is also beneficial when addressing clients that may not be compliant or appreciative of occupational therapy services, as my partner would always stand up for our profession and would never let a client speak poorly about occupational therapy. I improved my communication as well as advocation skills through working with my clinical instructor and physical therapy partner. As a future occupational therapist at an inpatient rotation, I gained the ability to communicate and advocate for the profession through an inter-professional situation. I am now more prepared to enter the workforce after completing this rotation. These are vital skills that I will carry into my career when I become a practicing occupational therapist in the medical field while working with other healthcare professionals.
Below is a comment on my Final Fieldwork Evaluation from my clinical instructor:

4. Assumes responsibility for professional behavior and growth, in accordance with AOTA standards.
To assume responsibility for one's professional behavior and growth is a key skill that a future occupational therapist must be able to recognize in order to become successful. While at my outpatient pediatric rotation, I began my rotation on a bit of a rough patch due to the culture shock that came when working with clients with more traumatic medical conditions, and the expectations that came with working for prestigious children's hospital. There was a moment in my rotation where I was at a failing standard and my clinical instructors had presented this to me in hopes that I could improve my skills. Instead of allowing myself to fall short of the expectations I had set for myself and the ones placed upon me by my clinical instructors, I contacted my academic fieldwork coordinator to begin taking the right steps to overcome my deficits and we initiated a learning contract to individually target the concerns from my clinical instructors. From this learning contract there was a short and long term goal for each behavior that needed to be addressed before the end of my outpatient pediatric rotation. As a student that was so close to finishing this was a heavy toll on my mindset and motivation, but I made sure to prevail and not let this learning contract be viewed as a negative mark on my journey to graduation. Each week, I made sure to put in the effort to improve my medical terminology, task analysis, articulation of therapeutic actives, and finally to relate occupational performance to biomechanics/anatomy. To provide evidence when achieving my short and long term goals based on my targeted behaviors, I had kept the comments made by my clinical instructors when provided critiques and had taken the time outside of clinic hours to create a task analysis form with activities that I could incorporate into my chosen client's treatment sessions. Towards the end of my rotation period, I had successful completed all aspects required of me on my learning contract and passed my midterm and final evaluation for LeBonheur Outpatient. I was proud of myself for assuming responsibility and not allowing self-doubt to hinder my success. Though some may take this learning contract as a deem of failure, I as a future occupational therapist let it motivate and guide me to becoming a better version of myself that I had not thought was possible.
To assume responsibility for one's professional behavior and growth is a key skill that a future occupational therapist must be able to recognize in order to become successful. While at my outpatient pediatric rotation, I began my rotation on a bit of a rough patch due to the culture shock that came when working with clients with more traumatic medical conditions, and the expectations that came with working for prestigious children's hospital. There was a moment in my rotation where I was at a failing standard and my clinical instructors had presented this to me in hopes that I could improve my skills. Instead of allowing myself to fall short of the expectations I had set for myself and the ones placed upon me by my clinical instructors, I contacted my academic fieldwork coordinator to begin taking the right steps to overcome my deficits and we initiated a learning contract to individually target the concerns from my clinical instructors. From this learning contract there was a short and long term goal for each behavior that needed to be addressed before the end of my outpatient pediatric rotation. As a student that was so close to finishing this was a heavy toll on my mindset and motivation, but I made sure to prevail and not let this learning contract be viewed as a negative mark on my journey to graduation. Each week, I made sure to put in the effort to improve my medical terminology, task analysis, articulation of therapeutic actives, and finally to relate occupational performance to biomechanics/anatomy. To provide evidence when achieving my short and long term goals based on my targeted behaviors, I had kept the comments made by my clinical instructors when provided critiques and had taken the time outside of clinic hours to create a task analysis form with activities that I could incorporate into my chosen client's treatment sessions. Towards the end of my rotation period, I had successful completed all aspects required of me on my learning contract and passed my midterm and final evaluation for LeBonheur Outpatient. I was proud of myself for assuming responsibility and not allowing self-doubt to hinder my success. Though some may take this learning contract as a deem of failure, I as a future occupational therapist let it motivate and guide me to becoming a better version of myself that I had not thought was possible.

5. Functions autonomously and effectively in a broad array of service models.
During one of the last remaining weeks I had at my inpatient rotation, my clinical instructor had to step-out for the day. I was tasked to handle my caseload as independently. I planned to spend the day the same as I had always, instead I was about to embark on a different journey with no assistance from my clinical instructor. I gathered all of my learned skills throughout these past weeks to put them into use. The day before my clinical instructor and I collaborated the schedule in order to met all of the patients on my caseload with the least amount of appointment conflicts and thus allowing a minimal need to rearrange while I was alone. On the schedule the first client I had, was not fond of receiving occupational therapy services nor did they have a desire to being admitted into an inpatient hospital. This client did not allow me to be present when they were completing any of their activities of daily living consisting of dressing, bathing, or toileting which ethically I could not charge time spent with them during their allotted time period. I used my therapeutic use of self to allow the client as much time as I could in order to salvage some bit of rapport with them. However, the hour time frame was nearing to an end and due to other appointment constraints I had to autonomously make a hard decision. As terrified as I was, I was straight forward with this client then informed them of the hospital's therapy policies and the consequences on the side of insurance if this patient did not attend their minimal required minutes. I had done this action all on my own and without any moral support from my clinical instructor. However, I effectively explained the situation to the client and made sure that I emphasized the purpose behind maintaining the minimal required minutes from the perspective of a client. After I had discussed the situation with the client, they did finally allow transportation to the therapy gym in order to receive the services that they required for the day.
Below is a discussion board post from my experience:
During one of the last remaining weeks I had at my inpatient rotation, my clinical instructor had to step-out for the day. I was tasked to handle my caseload as independently. I planned to spend the day the same as I had always, instead I was about to embark on a different journey with no assistance from my clinical instructor. I gathered all of my learned skills throughout these past weeks to put them into use. The day before my clinical instructor and I collaborated the schedule in order to met all of the patients on my caseload with the least amount of appointment conflicts and thus allowing a minimal need to rearrange while I was alone. On the schedule the first client I had, was not fond of receiving occupational therapy services nor did they have a desire to being admitted into an inpatient hospital. This client did not allow me to be present when they were completing any of their activities of daily living consisting of dressing, bathing, or toileting which ethically I could not charge time spent with them during their allotted time period. I used my therapeutic use of self to allow the client as much time as I could in order to salvage some bit of rapport with them. However, the hour time frame was nearing to an end and due to other appointment constraints I had to autonomously make a hard decision. As terrified as I was, I was straight forward with this client then informed them of the hospital's therapy policies and the consequences on the side of insurance if this patient did not attend their minimal required minutes. I had done this action all on my own and without any moral support from my clinical instructor. However, I effectively explained the situation to the client and made sure that I emphasized the purpose behind maintaining the minimal required minutes from the perspective of a client. After I had discussed the situation with the client, they did finally allow transportation to the therapy gym in order to receive the services that they required for the day.
Below is a discussion board post from my experience:

6. Upholds the AOTA Code of Ethics in practice.
Regardless of the clinical rotation site that I was placed at, I always would uphold and maintain the AOTA code of ethics while in practice. There was never a situation in which there was a breech of ethics during either of my two rotations, however there were times when a client I was currently treating in the inpatient hospital would ask about another client's medical condition or plan of care. I would simply inform the client I was working with that I was unable to answer personal information and if they wanted to communicate with the other person, then they are more than welcomed to do so in order to get clearance from the client themselves. Usually in this situation the client would be more than understanding of the rules. These patients do not have to follow guidelines when requesting personal information as they are not required to maintain health information privacy as I would. It may seem from another perspective as an innocent or even kind way of reaching out to others that need help, however as a future occupational therapist I still have to upload the code of ethics within any and all situations regardless of the intensions.
Below is a comment on my Final Fieldwork Evaluation from my clinical instructors:
Regardless of the clinical rotation site that I was placed at, I always would uphold and maintain the AOTA code of ethics while in practice. There was never a situation in which there was a breech of ethics during either of my two rotations, however there were times when a client I was currently treating in the inpatient hospital would ask about another client's medical condition or plan of care. I would simply inform the client I was working with that I was unable to answer personal information and if they wanted to communicate with the other person, then they are more than welcomed to do so in order to get clearance from the client themselves. Usually in this situation the client would be more than understanding of the rules. These patients do not have to follow guidelines when requesting personal information as they are not required to maintain health information privacy as I would. It may seem from another perspective as an innocent or even kind way of reaching out to others that need help, however as a future occupational therapist I still have to upload the code of ethics within any and all situations regardless of the intensions.
Below is a comment on my Final Fieldwork Evaluation from my clinical instructors:


7. Serves as a role model for honesty, integrity, and morally grounded decision making.
A client within the outpatient pediatric population could have a variety of strengths and weaknesses that can have a major or minor impact on specific age appropriate daily activities of living. There are situations when a client has concerns presented during an evaluation that are not within my scope of practice. I had to ethically provide them with the resources that would better suit their needs. There was one instance where I made a tough decision with my clinical instructor. We had to determinewhat the best cause of action would be for this client that we had seen for a feeding evaluation. This client had originally been referred for a possible physiological fear of eating non preferred foods and thus my clinical instructor and I were already prepared for the situation we had to face. During the history portion of the evaluation, the caregiver had reported concerns with the client not being able to eat a better array of healthy foods. This was a very common report given from caregivers with patients around at this age. However, as the evaluation progressed the caregiver described the way in which the client responded to non preferred foods. The report consisted of them being able to self feed, but then immediately vomiting afterwards. The client was then set-up for the feeding portion of the eval. My clinical instructor and I were prepared for anything to happen if the client were to become overwhelmed while eating. In this portion, I had presented foods that the client is known to prefer and then slowly and individually introducing foods that may not be as tolerated. The client responded well with each preferred food and even independently engaged with a newly introduced food that caregiver reported they would have never tried. Though there were no concerns regarding sensory processing with feeding, I made sure to educate the caregiver on my role as an occupational therapist and recommended psychological therapeutic services in order to address issues with anxiety while eating. I was honest with the caregiver and gave full integrity through my decision making process as I had not before treated a client with this specific concerns regarding eating. I explained that though I wanted to address these issues, I was not professionally equipped to handle. As a future occupational therapist it was of upmost importance to reassurance the caregiver's reports of concerns while also maintaining a morally grounded mindset to understand where the scope of practice begins and ends within the profession.
Below is a discussion board post from my experience:
A client within the outpatient pediatric population could have a variety of strengths and weaknesses that can have a major or minor impact on specific age appropriate daily activities of living. There are situations when a client has concerns presented during an evaluation that are not within my scope of practice. I had to ethically provide them with the resources that would better suit their needs. There was one instance where I made a tough decision with my clinical instructor. We had to determinewhat the best cause of action would be for this client that we had seen for a feeding evaluation. This client had originally been referred for a possible physiological fear of eating non preferred foods and thus my clinical instructor and I were already prepared for the situation we had to face. During the history portion of the evaluation, the caregiver had reported concerns with the client not being able to eat a better array of healthy foods. This was a very common report given from caregivers with patients around at this age. However, as the evaluation progressed the caregiver described the way in which the client responded to non preferred foods. The report consisted of them being able to self feed, but then immediately vomiting afterwards. The client was then set-up for the feeding portion of the eval. My clinical instructor and I were prepared for anything to happen if the client were to become overwhelmed while eating. In this portion, I had presented foods that the client is known to prefer and then slowly and individually introducing foods that may not be as tolerated. The client responded well with each preferred food and even independently engaged with a newly introduced food that caregiver reported they would have never tried. Though there were no concerns regarding sensory processing with feeding, I made sure to educate the caregiver on my role as an occupational therapist and recommended psychological therapeutic services in order to address issues with anxiety while eating. I was honest with the caregiver and gave full integrity through my decision making process as I had not before treated a client with this specific concerns regarding eating. I explained that though I wanted to address these issues, I was not professionally equipped to handle. As a future occupational therapist it was of upmost importance to reassurance the caregiver's reports of concerns while also maintaining a morally grounded mindset to understand where the scope of practice begins and ends within the profession.
Below is a discussion board post from my experience:

