1. Invests in the acquisition of evidence through participation in workshops, continued education and pursuit of additional degrees.
During my outpatient pediatric rotation, every last Wednesday of the month there was a meeting held with all the therapists from the downtown and east locations to engage in team building activities or report recent updates on facility procedures. At one of the most recent meetings, two physical therapists from the east location presented an in-service workshop on rib cage mobility and treatment session implementation. This in-service focused on the ways that we as therapists could promote increased postural control and functional reaching for clients with neuromuscular diagnosis such as Cerebral Palsy. It was a well informed in-service that placed focus onto more basic and foundational components that are required in order to have a greater performance level in our gross motor movements, occupations, and social interactions. If the client has a tight chest they will be unable to complete functional reaching or maintain the core strength required as proximal stability creates distal mobility. The physical therapist went through each area of the rib cage that could be addressed and provided the outcomes that we should expect to see when performing on our clients. Since the location of this type of muscle facilitation was around vital organs, the physical therapists presenting this in-service made sure to explain how to safely perform these stretches on clients who had gastronomy tubes and tracheostomies in order to prevent any further injuries to those sensitive areas. We were paired up and had to practice on each other to better understand the pressure and control that it required to properly complete rib cage mobility movements. I really enjoyed this workshop as I had a client on my caseload that was diagnosed with Cerebral Palsy and would greatly benefit from this form of facilitation. I spent time to thoroughly invest in the acquisition of emerging evidence based practice through this in-service to continue my life long pursuit of obtaining knowledge that will better the interventions that I provide to my future clients as an occupational therapist.
During my outpatient pediatric rotation, every last Wednesday of the month there was a meeting held with all the therapists from the downtown and east locations to engage in team building activities or report recent updates on facility procedures. At one of the most recent meetings, two physical therapists from the east location presented an in-service workshop on rib cage mobility and treatment session implementation. This in-service focused on the ways that we as therapists could promote increased postural control and functional reaching for clients with neuromuscular diagnosis such as Cerebral Palsy. It was a well informed in-service that placed focus onto more basic and foundational components that are required in order to have a greater performance level in our gross motor movements, occupations, and social interactions. If the client has a tight chest they will be unable to complete functional reaching or maintain the core strength required as proximal stability creates distal mobility. The physical therapist went through each area of the rib cage that could be addressed and provided the outcomes that we should expect to see when performing on our clients. Since the location of this type of muscle facilitation was around vital organs, the physical therapists presenting this in-service made sure to explain how to safely perform these stretches on clients who had gastronomy tubes and tracheostomies in order to prevent any further injuries to those sensitive areas. We were paired up and had to practice on each other to better understand the pressure and control that it required to properly complete rib cage mobility movements. I really enjoyed this workshop as I had a client on my caseload that was diagnosed with Cerebral Palsy and would greatly benefit from this form of facilitation. I spent time to thoroughly invest in the acquisition of emerging evidence based practice through this in-service to continue my life long pursuit of obtaining knowledge that will better the interventions that I provide to my future clients as an occupational therapist.

|

|
2. Is a knowledgeable consumer of global research related to occupational therapy and utilizes an evidence based approach to practice.
For a patient who has suffered a stroke there is an abundance of research that can be utilized to provide an evidence based approach to the practice of occupational therapy. At the start of my inpatient rotation, I had a patient on my caseload who had lost a majority of function on one side of their body. This patient was unable to communicate effectively for the few times that I worked with them. In comparison to the other patients on my caseload at the time, this patient required a more individualized approach to treatment and performance with daily activities of living. My clinical instructor used their expertise to base the client's interventions on tasked-oriented approaches which focused on the patient using their affected side to complete various tasks. I took it upon my self as a future occupational therapist to really dive into this therapeutic approach to treating a client who had suffered a stroke with a heavily affected side. I learned through this article that a task-oriented therapy approach applies motor learning , which includes the requirements of the tasks, and motor control of the body parts involved. Through this experience I too have become a knowledgeable consumer of the global research related to occupational therapy and I have been able to recognize the use of and implementation of this evidence based approach in practice through my clinical instructor.
Below is a discussion board post from my experience:
For a patient who has suffered a stroke there is an abundance of research that can be utilized to provide an evidence based approach to the practice of occupational therapy. At the start of my inpatient rotation, I had a patient on my caseload who had lost a majority of function on one side of their body. This patient was unable to communicate effectively for the few times that I worked with them. In comparison to the other patients on my caseload at the time, this patient required a more individualized approach to treatment and performance with daily activities of living. My clinical instructor used their expertise to base the client's interventions on tasked-oriented approaches which focused on the patient using their affected side to complete various tasks. I took it upon my self as a future occupational therapist to really dive into this therapeutic approach to treating a client who had suffered a stroke with a heavily affected side. I learned through this article that a task-oriented therapy approach applies motor learning , which includes the requirements of the tasks, and motor control of the body parts involved. Through this experience I too have become a knowledgeable consumer of the global research related to occupational therapy and I have been able to recognize the use of and implementation of this evidence based approach in practice through my clinical instructor.
Below is a discussion board post from my experience:

3. Integrates individual clinical expertise and patient values with the best available external clinical evidence.
At my outpatient pediatric rotation, I integrated my individual clinical expertise with my patient's values while utilizing resourceful external clinical evidence in order to promote motivation and engagement for the functional task. I had a patient with Cerebral Palsy that I would co-treat with physical therapy every week. The main focus would be centered on basic foundations of developmental milestones to increase the patient's independence in age appropriate play. This patient had been attending therapy services with my clinical instructor before I had begun my rotation and typically had a harder time in maintaining attention to demanded tasks due to a lack of overall motivation. The patient's lack of motivation would then lead them to demonstrate poor posture. The patient would use their entire body to curl into a flexor pattern and they lacked proximal stability needed for distal mobility. I used my fingers to stroke the extensor muscles on their neck and back while the physical therapist would provide stabilization at the trunk and hips to promote postural control. However, over time the patient would not respond with any change in posture. During one of our treatment sessions when the physical therapist and I had ran out of ideas on how to encourage the patient to participate, my clinical instructor had suggested the use of vibrations to stimulate their extensor muscles. After applying a vibrating cushion under the patient's hips an a vibration citer-stick to their spine and neck, they immediately went into full extension and demonstrated greatly improved motivation to the demanded tasks. I took the liberty to use my evidence based practice skills to find an article to support this discovery made during my session and found that vibration is a highly effective technique used on children with Cerebral Palsy to increase postural control and overall motor function. I was able to integrate the clinical expertise that I possessed while considering the patient's values with the use of effective external clinical evidence.
Below is a discussion board post from my experience:
At my outpatient pediatric rotation, I integrated my individual clinical expertise with my patient's values while utilizing resourceful external clinical evidence in order to promote motivation and engagement for the functional task. I had a patient with Cerebral Palsy that I would co-treat with physical therapy every week. The main focus would be centered on basic foundations of developmental milestones to increase the patient's independence in age appropriate play. This patient had been attending therapy services with my clinical instructor before I had begun my rotation and typically had a harder time in maintaining attention to demanded tasks due to a lack of overall motivation. The patient's lack of motivation would then lead them to demonstrate poor posture. The patient would use their entire body to curl into a flexor pattern and they lacked proximal stability needed for distal mobility. I used my fingers to stroke the extensor muscles on their neck and back while the physical therapist would provide stabilization at the trunk and hips to promote postural control. However, over time the patient would not respond with any change in posture. During one of our treatment sessions when the physical therapist and I had ran out of ideas on how to encourage the patient to participate, my clinical instructor had suggested the use of vibrations to stimulate their extensor muscles. After applying a vibrating cushion under the patient's hips an a vibration citer-stick to their spine and neck, they immediately went into full extension and demonstrated greatly improved motivation to the demanded tasks. I took the liberty to use my evidence based practice skills to find an article to support this discovery made during my session and found that vibration is a highly effective technique used on children with Cerebral Palsy to increase postural control and overall motor function. I was able to integrate the clinical expertise that I possessed while considering the patient's values with the use of effective external clinical evidence.
Below is a discussion board post from my experience:

4. Applies the domain of occupational therapy in gathering, evaluating, setting goals, planning and implementing occupational therapy.
Throughout my outpatient pediatric rotation I used the domain of occupational therapy to gather, evaluate, and set goals in order to implement relevant information into my sessions. I utilized the Peabody Developmental Motor Scales, Second Edition (PDMS-2) assessment during an evaluation session with a client that was referred for occupational therapy services. I used the PDMS-2 to gather information to see if they are age appropriate within their developmental milestones. With the assessment I evaluated the fine and visual motor integration skills that the client met and what skills needed to be further addressed. The PDMS-2 was an accurate tool that I used to create an outline in order to set goals for my evaluated clients on my caseload. I would use the assessment to create interventions and broke tasks down into preparatory and purposeful activities. I planned and implanted these activities into each session I had with my clients by initially starting off with the preparatory tasks to have them understand the basic concepts. Then, once they mastered the task, I transferred those learned preparatory skills to carry over onto the functional task that will address the client's goals. The PDMS-2 was an effective tool for a future occupational therapist to apply the domain of occupational therapy in the outpatient pediatric setting.
Throughout my outpatient pediatric rotation I used the domain of occupational therapy to gather, evaluate, and set goals in order to implement relevant information into my sessions. I utilized the Peabody Developmental Motor Scales, Second Edition (PDMS-2) assessment during an evaluation session with a client that was referred for occupational therapy services. I used the PDMS-2 to gather information to see if they are age appropriate within their developmental milestones. With the assessment I evaluated the fine and visual motor integration skills that the client met and what skills needed to be further addressed. The PDMS-2 was an accurate tool that I used to create an outline in order to set goals for my evaluated clients on my caseload. I would use the assessment to create interventions and broke tasks down into preparatory and purposeful activities. I planned and implanted these activities into each session I had with my clients by initially starting off with the preparatory tasks to have them understand the basic concepts. Then, once they mastered the task, I transferred those learned preparatory skills to carry over onto the functional task that will address the client's goals. The PDMS-2 was an effective tool for a future occupational therapist to apply the domain of occupational therapy in the outpatient pediatric setting.

|

|
5. Contributes to the knowledge base of OT practice by mentoring students, performing research, publishing, presenting and/or teaching.
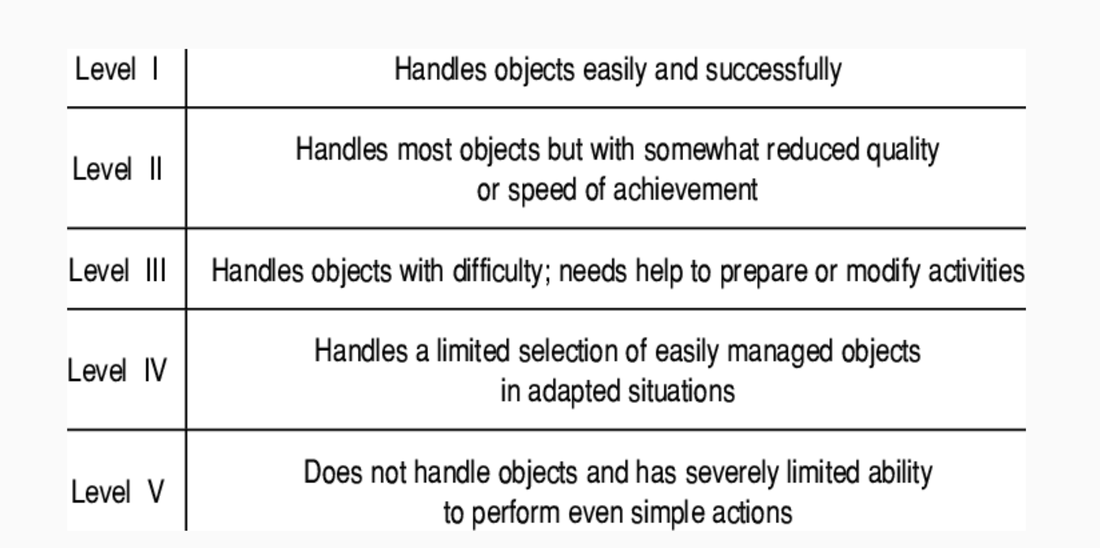
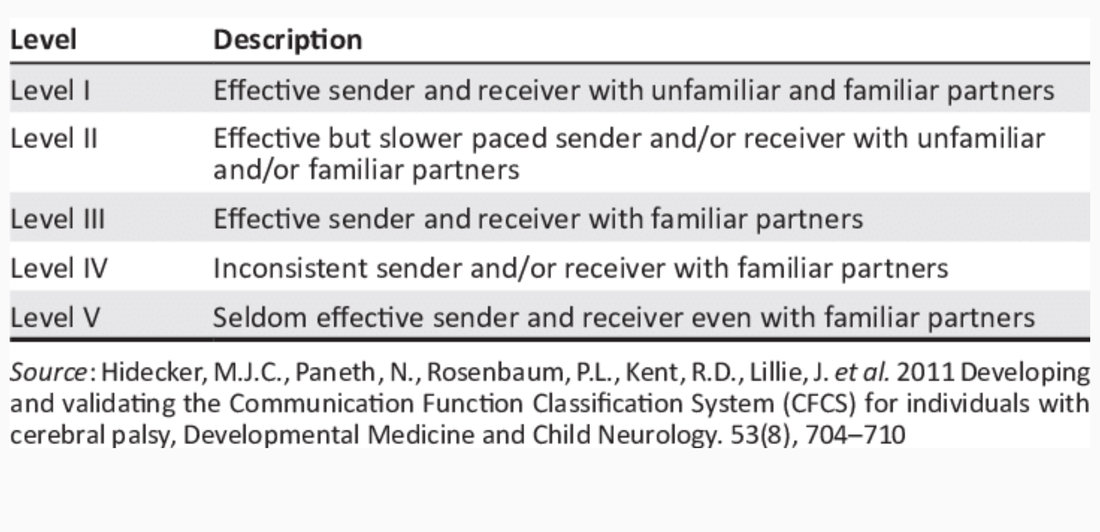
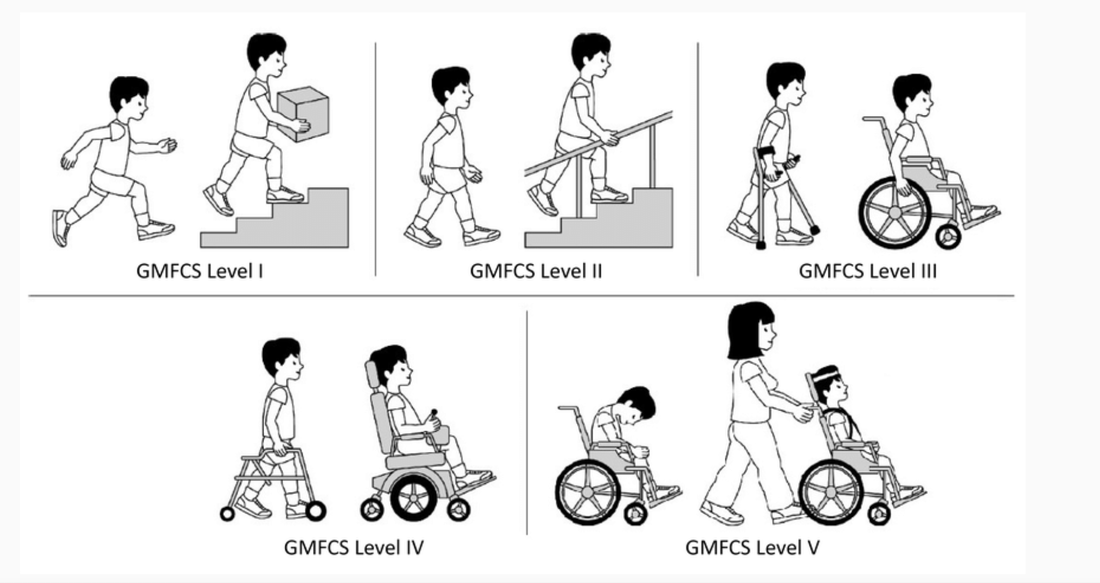
While at my outpatient pediatric outpatient rotation I contributed to the knowledge base of occupational therapy practice through presenting an inservice. This inservice focused on providing resources for therapists to use with patients on their caseload that were diagnosed with Cerebral Palsy. I used this inservice to provide the therapists at my outpatient pediatric rotation with classifications systems designed to evaluate different skills of children diagnosed with Cerebral Palsy. There are three classification systems that are most commonly used by therapists when working with this patient population. The Communication Function Classification System, the Manual Ability Classification System, and the Gross Motor Function Classification System. They are each used to determine the current level of communication, bilateral hand coordination, and motor skills of a child with Cerebral Palsy. The purpose of this inservice was to provide the therapists with a collective of these classification systems to contribute to their current knowledge base of occupational therapy practice.
While at my outpatient pediatric outpatient rotation I contributed to the knowledge base of occupational therapy practice through presenting an inservice. This inservice focused on providing resources for therapists to use with patients on their caseload that were diagnosed with Cerebral Palsy. I used this inservice to provide the therapists at my outpatient pediatric rotation with classifications systems designed to evaluate different skills of children diagnosed with Cerebral Palsy. There are three classification systems that are most commonly used by therapists when working with this patient population. The Communication Function Classification System, the Manual Ability Classification System, and the Gross Motor Function Classification System. They are each used to determine the current level of communication, bilateral hand coordination, and motor skills of a child with Cerebral Palsy. The purpose of this inservice was to provide the therapists with a collective of these classification systems to contribute to their current knowledge base of occupational therapy practice.

|
|
6. Incorporates continued education as a lifelong practice with the commitment to remain up-to-date and well-informed.
While at my outpatient pediatric rotation, I presented an in-service on emerging treatments within the medical field in regards to rehabilitation services related to the outpatient pediatric setting. When I gathered data for this in-service, I discovered a newly proposed evidence based practice for children who were diagnosed with Cerebral Palsy. I found a systematic review of the role and effects of hippotherapy for children with Cerebral Palsy. Within this article there were findings that supported the idea that this type of therapy approach would benefit in aspects of physical, social, and cognitive abilities for these children. I had previously seen hippotherapy while on my very first clinical rotation as a student, however there was little information at the time available for this specific population of diagnoses. During my in-service I presented this approach to the therapists at my outpatient pediatric rotation as a suggestion to provide for their clients in-between episodes. This intervention approach would give the patients a structured break to continue growing skills and prevent burnout. This in-service sparked a discussion within our department and inspired other therapists to research more on the topic of hippotherapy. I incorporated continued education as a lifelong practice to remain up to date and well informed not only for myself but for other clinicians at my outpatient pediatric rotation.
While at my outpatient pediatric rotation, I presented an in-service on emerging treatments within the medical field in regards to rehabilitation services related to the outpatient pediatric setting. When I gathered data for this in-service, I discovered a newly proposed evidence based practice for children who were diagnosed with Cerebral Palsy. I found a systematic review of the role and effects of hippotherapy for children with Cerebral Palsy. Within this article there were findings that supported the idea that this type of therapy approach would benefit in aspects of physical, social, and cognitive abilities for these children. I had previously seen hippotherapy while on my very first clinical rotation as a student, however there was little information at the time available for this specific population of diagnoses. During my in-service I presented this approach to the therapists at my outpatient pediatric rotation as a suggestion to provide for their clients in-between episodes. This intervention approach would give the patients a structured break to continue growing skills and prevent burnout. This in-service sparked a discussion within our department and inspired other therapists to research more on the topic of hippotherapy. I incorporated continued education as a lifelong practice to remain up to date and well informed not only for myself but for other clinicians at my outpatient pediatric rotation.

